

Author: Bourzac Katherine
Institution: Biology and Comparative Literature
Date: September 2005
In the wake of the October anthrax mailings, America has become attuned to the possibility of terrorists unleashing smallpox on the United States. Unlike anthrax, smallpox is highly contagious and difficult to contain. Although smallpox was eradicated from the United States in 1949 and officially eradicated worldwide in 1980, Americans are currently very vulnerable to the disease, which might spread rapidly throughout the United States - and to other countries - upon release.

article_528_order_0
Mandatory vaccination of school children against smallpox ended in 1972 in the United States. Because the last outbreak of smallpox in the United States was in February 1949, by 1972 the risk of vaccine complications far outweighed the risk of smallpox infection. An estimated 120 million Americans - about half the population - have never been vaccinated and have no immunity to the disease. Those who have been vaccinated have not had a booster shot in decades; their immunity has waned, although no one knows by what factor and how susceptible to smallpox they may be.
Because of its extreme virulence, smallpox has impacted not only the lives of its victims but even the outcomes of wars and conquests. Smallpox scourged the entire world before Dr. Edward Jenner invented vaccinations in the 18th century and the official eradication of the disease by the World Health Organization (WHO) occurred in 1980. If smallpox were reintroduced to the United States, many fear present-day Americans would fare no better than the Native Americans, whose numbers were devastated when Europeans introduced the disease to this continent in the 16th century. "Today, we're all Indians," says Elizabeth Fenn, historian and author of Pox Americana.
Though the situation is grave, Fenn's warning is probably overstated. Millions of Americans have been vaccinated; their immunity -- even if it has waned over time -- would slow the spread of the disease upon an outbreak. The government currently has more than 100 million doses of smallpox vaccine and has signed a contract to purchase enough to vaccinate all Americans in case of an outbreak. These new stocks should be ready by the end of the year, but the current supply would be enough to contain isolated outbreaks. Large-scale outbreaks of genetically altered smallpox would pose more of a problem for the government.
article_528_order_1
Since its eradication, debate has continued about whether U.S. and Russian smallpox stocks -- which were generated for bio-weapons research during the cold war -- should be destroyed, since their existence leaves open the possibility of smallpox falling into the hands of bioterrorists. North Korea, Iraq, and possibly other nations, have undeclared smallpox stockpiles. No matter what protective measures the government takes, a smallpox outbreak is possible as long as such stockpiles exist.
Smallpox Pathogenesis and Symptoms
Smallpox is contracted by inhalation of variola virus particles. Lesions in the throat and mouth release large amounts of virus into the saliva, which are spread into the air by coughing. Smallpox is spread via saliva during face-to-face contact or by inhalation of virus particles from pus and scabs encountered on bed sheets and other places.
Upon inhalation, variola implants itself in the lining of the throat and nasal cavity, and then migrates to the lymph nodes and the blood. By the eighth day after contraction, the virus has undergone intense multiplication. Variolae localize in blood vessels in the skin and inside the mouth and throat. After about 12-14 days of incubation, high fever, headache, backache, and other flu-like symptoms appear. A rash appears in the mouth and throat and on the face, arms, trunk, and legs. After one or two days, the rash turns into deeply imbedded pustules, or pox, which become scabby after about a week.
At this point, the pox do not itch, but they cause excruciating, fiery pain. Sometimes the pox are so numerous and close together that they cannot be distinguished from one another. In 1634, William Bradford, governor of the Plymouth colony in Massachusetts, wrote of the horrific effect of smallpox on the skin of infected Native Americans: "Their skin... cleaves... to the matts they lye on; when they turn them, a whole side will flea off at once... they die like rotten sheep." Viral toxins and human immune complexes circulating in the blood cause death in the second week of infection. The most virulent form of smallpox, caused by variola major, is fatal in 30-50% of unvaccinated patients. A milder form of smallpox, called alastrim, is caused by the variola minor strain and has only a 1% death rate among unvaccinated people. If the smallpox patient recovers, the scabs separate and fall off after three to four weeks, accompanied by extreme itching. The pox leave behind terrible scars, especially on the face.
According to the American Medical Association (AMA), smallpox occasionally causes encephalitis and blindness, but in its most common form it rarely affects organs other than the skin.
Variola is extremely virulent: The AMA says natural infection may occur after inhalation of fewer than 10 viral particles. Although the patient is most contagious during the first week, viral particles from saliva and sores remain viable outside the body for a long time - for instance, on sheets and clothing -- and may infect others months later.<
Smallpox in Human History
The ancestor of the variola virus jumped species from rodents to African hunters thousands of years ago. Over millennia, the rodent virus specialized to infect humans, then spread across Africa and beyond, menacing the entire globe. In the seventh and eighth centuries A.D., Arab armies carried smallpox out of Africa to Southwestern Europe; in the 11th and 13th centuries the crusades and trade along the Silk Road to China also contributed to the widespread dissemination of the disease across Eurasia and beyond.
According to Greek historian Thucydides's, variola is thought to be the cause of the 430 B.C. plague that weakened Athens and contributed to its defeat by Sparta. Smallpox facilitated the European conquest of North and South America. Native populations had never been exposed to variola virus and had no immunity to it. The Spaniards' victory over the Aztecs is a well-known example. In 1519, Spanish forces led by conquistador Hernando Cortes arrived in the Aztec capital of Tenochtitlan. The Aztecs were decimated two years after Cortes' arrival -- but not by the Spaniard's horses, guns, or military skill. It was smallpox that almost completely annihilated the Aztecs, causing the population to fall from 25 million in 1519 to three million 50 years later.
Smallpox also drastically affected everyday life. In 1800, English historian Thomas Macaulay wrote that the disease "was always present, filling the churchyard with corpses, tormenting with constant fears all whom it had not yet stricken ... making the eyes and cheeks of a betrothed maiden objects of horror to the lover." Between 1719 and 1746, London suffered five major smallpox outbreaks. As the 18th century drew to a close, smallpox was killing 400,000 Europeans each year and had spread from Eurasia to Australia, South Africa, and North and South America.
Vaccination
Inoculation against smallpox was first performed in India in 1000 B.C. Pus or scabs from variola pox were rubbed into a skin lesion in a process called variolation. Although variolation sometimes led to smallpox infection, it reduced the death rate among infected people from 30% to 1%. Lady Mary Wortley Montagu, the wife of a member of the English Parliament, observed variolation in the Ottoman court during a trip to Constantinople in 1717. She persuaded the Princess of Wales and her husband to sponsor a public experiment on the efficacy of variolation on prisoners. Due to the success of the experiment, the princess had her own children variolated. From then on, variolation became more widespread; however, because of medical and religious concerns it was not completely embraced by the public. The pus used for variolation was often contaminated with the bacteria that caused tuberculosis or syphilis. To cure people by infecting them seemed unnatural and immoral. However, due to variolation's dramatic reduction in smallpox death rates, the procedure spread across Europe and to America throughout the late 18th century.
In 1770, Dr. Edward Jenner, of Glouchestershire, England noticed that milkmaids who had been infected by cowpox (a much milder virus in the same genus as smallpox) had smooth complexions free of pox scars and didn't contract smallpox. To test his theory that cowpox immunity lessened the severity of smallpox, he variolated 13 milkmaids with smallpox who had had cowpox. Generally, a few pox would develop around the site of variolation, but the milkmaids he variolated in his study did not develop the characteristic lesions. In 1796, now confident in his theory that previous cowpox infection protected people from smallpox infection, Jenner performed a daring and highly unethical experiment: He injected a boy with cowpox, and then variolated him. Like the milkmaids in his previous experiments, the boy did not develop any smallpox lesions. Jenner coined the word vaccination (from Latin vacca, cow) to describe his cowpox inoculation. Jenner performed his experiments over 100 years before Pasteur advanced his germ theory of disease in 1880. Jenner did not know about immunity or viruses -- he only knew his vaccination worked.
Jenner's vaccination method was not widely accepted for several years. In 1797, the British Royal Society rejected a paper in which Jenner described his vaccination experiments. The members felt that his ideas were "too revolutionary" and his experimental evidence "too limited." Jenner published his paper privately in 1798; within the year it was translated into Latin, German, and French, and about 1000 people were vaccinated.
article_528_order_2
Jenner's method of cowpox inoculation, called vaccination, became more and more popular in Europe and America over the next 50 years, largely because it had much milder side effects than variolation and could never result in smallpox infection. Variolation involves exposing patients to variola virus; vaccination only exposes patients to cowpox. By 1800, more than 100,000 citizens of Great Britain had been vaccinated and in 1840 the British Parliament passed the Vaccination Act, mandating free vaccination of infants and outlawing variolation. Most Western governments adopted similar laws by 1900. In 1939, Allan Downie of the University of Liverpool determined that the virus used for smallpox vaccinations was no longer genetically identical to cowpox but had diverged into a new virus. Downie called the virus vaccinia. To this day no one knows why the change occurred.
In the United States, rates of smallpox infection decreased as mandatory vaccination of schoolchildren was put in place throughout the first half of the 20th century and the invention of the ice box made vaccine storage efficient. While the United States and European countries were getting smallpox under control, the developing world still suffered from it. Infection rates were high in Africa, South America, and Asia, where vaccination was not as widespread as in the West. During World War II, smallpox infection swelled. Previously unexposed regions were overtaken by variola carried by foreigners, or by soldiers who brought the virus home from foreign lands. From 1941 to 1946, the percentage of countries in which smallpox was endemic rose from 69% to 87%. During that period, smallpox killed three to four million people annually.
Worldwide Eradication

article_528_order_3
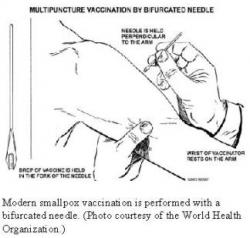
On January 1, 1967, the WHO began the Intensified Smallpox Eradication Program, one of the greatest triumphs in the history of medicine. The WHO employed a strategy of mass vaccination coupled with subsequent surveillance and containment. After mass vaccination of a population, WHO agents monitored it for isolated cases of smallpox, containing them via quarantine and small-scale vaccination. Key to the program's success was its sensitivity to local needs. Operations were specialized to each country and agents worked carefully within the framework of local cultures. Freeze-dried vaccine (which does not require refrigeration) and a hydraulically powered jet injector capable of performing 1000 vaccines per hour made eradication possible in developing countries where electricity was scarce and generators unreliable. The last reported case of smallpox occurred in Somalia in 1977; the disease was declared eradicated and large-scale vaccination ended worldwide in 1980.
American and Soviet Germ Warfare Programs

article_528_order_4
The U.S. Army began germ warfare research in 1942 in response to intelligence about Tokyo and Berlin's germ warfare programs. George Merck (of Merck pharmaceuticals) was put in charge of bioweapons research at the U.S. Army base at Fort Detrick, Maryland. The program started out with an emphasis on bacterial rather than viral agents. For example, in the 1950s, according to Germs: Biological Weapons and America's Secret War, Fort Detrick scientists worked to determine how much anthrax was necessary to annihilate Moscow, Kiev, and Leningrad.
In 1956, the U.S. government learned of the existence (but not the extent) of the Soviet bioweapons program and expanded its program in response, shifting its emphasis from bacterial to viral disease. U.S. scientists began freeze-drying smallpox and testing aerosol generators for dissemination. The generators were designed for hiding in everyday objects. Atomizers hidden in briefcases were tested with mock smallpox germs in the then-named Washington International Airport in May 1965. Scientists determined that if the virus had been real, one in 12 travelers would have been infected. In the 1960s, the Army secretly considered using smallpox as a weapon against the North Vietnamese but decided against it because of the risk of Soviet retaliation in kind.
On November 25, 1969, then-President Nixon ended America's biological warfare program because he felt the human race already carried "too many of the seeds of its own destruction." His administration led the world in advocating the 1972 Biological and Toxic Weapons Convention treaty, which banned possession of such agents except for research into vaccines and treatments. The United States and the Soviet Union were among the approximately 100 countries to sign.
The American government did not know the tremendous scale on which the Soviet government pursued its bioweapons operations until October 1989, when Soviet scientist Vladimir Pasechnik defected to Great Britain and detailed what he knew. The Soviet operation had been underway since 1928 but began in earnest in 1967 when the government sent agents to India during a smallpox outbreak. Soviet doctors inoculated and treated patients while the KGB obtained samples of the virus, an especially virulent strain of variola major. When the WHO certified the global eradication of smallpox in 1980, Soviet officials knew it would be an excellent biological weapon.
The Soviet Union researched efficient means of growing and delivering variola. They intended to use smallpox to achieve total annihilation in case of nuclear warfare with the United States and worked on a device to attach to nuclear warheads that would disseminate variola virus. Scientists searched for chemicals to stabilize the virus in a radioactive environment so that it might infect and kill any American survivors of nuclear holocaust.
U.S. germ warfare projects began more than 10 years after the Soviet Union's and on a much smaller scale. However, the U.S. Army's program was atrocious in its own right. At its peak production level, the Soviet Union produced 100 metric tons of variola virus annually with a combined peak yearly production of biowarfare agents (including bubonic plague and anthrax) of 10,000 metric tons. The U.S. Army never mass-produced variola or bubonic plague for germ warfare. Its combined peak production of other biowarfare agents like anthrax was 6.5 metric tons per year. The Army tested its germ weapons on prisoners in Ohio State Penitentiary and on nearly a thousand soldiers in the Utah desert, also spraying civilians with "mild germs" in order to investigate delivery techniques.
The Fate of Smallpox Stockpiles
Many fear that the retention of variola stocks by the United States and Russia puts us in danger of smallpox attack. In addition to Russia and the United States, North Korea and Iraq are suspected to have stockpiles of variola major. Rogue nations or terrorists may have a virulent strain of smallpox, obtained from an American or Soviet lab working on biological warfare. Financial support for Russian laboratories has declined in the past few years, leaving their stocks particularly vulnerable, according to the AMA. While the stocks exist, it is possible for terrorists to steal and use them. One of the primary arguments against retaining the American and Russian stocks of virus is the possibility that terrorists will use the retention as an excuse to develop weapons of biological warfare. Virologist Jeffrey Almond of the University of Reading (UK) would "argue for the preservation of smallpox" for research if we lived in "an ideal world," but as things stand, we should destroy our stocks to make it clear that "it's a crime against humanity to develop such weaponry."
Some feel that to destroy Soviet and American stocks of the virus and declare it eradicated from Earth would be perpetrating a fraud. Iraq and North Korea have undeclared variola stocks and reports of uncertain reliability suggest that China, Cuba, India, Iran, Israel, Pakistan, and Yugoslavia may also have stocks. Any country might have obtained and saved samples of the virus from infected patients before smallpox was eradicated.
Due to the risks of retaining the virus, in 1996 the WHO set mid-1999 as the date for destruction of all variola stocks. Decades of presidential administrations have supported the destruction of U.S. variola stockpiles. The Clinton administration "privately assured" other nations it would support destruction in 2002 after further research, and together with Russia pushed the WHO to extend the deadline.
However, the political climate has changed since September 11 -- the possibility of a bioterror attack has become more palpable, even if the probability of such an attack has not actually increased. Kenneth Bernard, former U.S. assistant surgeon general, believes research on variola stocks is critical. In an Associated Press story from January 17, 2002, he said, "We regard the potential release of smallpox as a critical national and international security issue."
That same day, the WHO reversed its order, recommending the retention of variola for research into new vaccines and treatments. No new date was set for the destruction of the viral stockpiles, although research progress reports are to be drawn up in two to three years. China was the only nation to protest the indefinite extension of the destruction deadline. China's ambassador to the WHO, Sha Zukang, said in the same Associated Press article that China believes "early eradication of the virus stocks is the only fundamental guarantee of the eradication of smallpox."
The Bush administration recently announced that U.S. variola stocks will not be destroyed until scientists develop two antiviral drugs and a vaccine all Americans can safely take (including those with suppressed immune systems). Bush proposed a $3.7 billion increase in the National Institutes of Health (NIH) budget for the next fiscal year, which begins October 1. The NIH bioterror defense research budget will increase five-fold to $1.5 billion. In a January 25, 2002 Los Angeles Times story, Dr. Anthony Fauci, infectious disease chief at NIH, was recorded as saying research priorities will include developing a better smallpox vaccine and quicker methods of diagnosing smallpox. The increase worries many analysts, government officials, and scientists, who wonder whether the money will be spent wisely and whether it will unnecessarily detract from more immediate problems such as the flu, which kills more than 15,000 Americans in a typical season. Proposed NIH bioterror research will focus on anthrax and smallpox, but this may leave the United States vulnerable to many other deadly agents. Many feel that more of the money should go toward public health efforts, including better training for doctors and more hospital beds. Such measures would benefit more people no matter what kind of bioterrorist attack may occur.
American Preparedness Against the Threat of Terrorism
It is difficult to predict the likelihood of a terrorist smallpox attack on the United States. As long as stockpiles exist, an attack is possible. The worst-case scenario is bleak: Officials might not be able to contain a wide-spread outbreak of a genetically-engineered virus without large numbers of casualties, although a major epidemic would probably not ensue. If non-genetically-engineered smallpox were unleashed in the United States on a small scale - which is much more likely - casualties would be relatively low: Existing immunity in the populace and vaccine supply would probably protect a majority of the population.
New studies imply that immunity may last longer than previous estimates, which guaranteed immunity for only a decade after vaccination. An article by Joe Cohen in a recent issue of Science magazine describes three such studies. A study by Israeli researcher Baruch El-Ad showed a decline in antibody levels for three years after vaccination but a constant level of antibodies for the next 30 years. Francis Ennis of the University of Massachusetts medical school found that virus-specific T-cell memory can persist for up to 50 years "in presumed absence of antigen." T-cell memory allows the body to "remember" an antigen like a viral protein so that, if exposed to it in the future, the immune system can react quickly to stifle infection. A study published in 1913 by William Hanna examined the severity and fatality of smallpox in people of various ages who were immunized only once in infancy. These data show that 93% of people ages 50 years and older who were immunized in infancy escaped severe infection and death while 50% of unimmunized people in the same age group suffered severe illness and died.
As the response of New York officials to the last American smallpox outbreak in 1947 illustrates, mass vaccination is wasteful and dangerous. Reacting to public hysteria, officials vaccinated 6 million people in one month according to a November 6, 2001 Los Angeles Times story, exhausting the vaccine supply in the area.
Containment of the last smallpox case in America in 1962 was more successful and achieved by much more moderate means. James Orr had flown from Brazil to New York, and then took a train to Toronto, before coming down with smallpox. Rather than sealing the U.S.-Canadian border and vaccinating millions of people, officials vaccinated only 3,000 people who had been in the same area as the infected man and fumigated the planes and trains. When the public health system reacts quickly to a smallpox outbreak affecting a relatively small number of people, fewer need to be vaccinated.
On November 28, 2001, the Department of Health and Human Services signed a contract with biotech firm Acambis Inc. to buy 155 million doses of smallpox vaccine within a year, bringing the U.S. stockpile of the vaccine to 286 million doses. However, because of the risk of complications , the vaccine will not be used unless an outbreak occurs: If all Americans were vaccinated, 400 people would most likely die from complications, 250 people would contract a potentially fatal rash, and three out of every one million would contract encephalitis. Scientists at four American research universities are also studying the effects of diluting vaccines to one-fifth and one-tenth strength. If these doses are strong enough to generate immunity, a smallpox outbreak could be contained with a limited amount of vaccine.
Vaccination efforts are important but would fail to contain the disease unless coupled with an effective quarantine, which could be difficult to achieve: The incubation period of smallpox is about 12 days (giving infected individuals time to scatter far from the infection site) and the disease is difficult to diagnose for the first two to three days, because the symptoms are flu-like. One can imagine a worst-case scenario in which terrorists discharge variola virus into a crowded public area; exposed people would scatter, perhaps across the country and around the world if the attack occurred at an airport. Infection rates would vary, depending on the age group of exposed people (i.e., whether they have been vaccinated and how long ago), but people would not show symptoms until 12 days after the exposure. Once they began to manifest symptoms of infection, people might be misdiagnosed for 2-3 days, further delaying initiation of quarantine efforts.
Senior officials in the Clinton administration all but failed a role-playing exercise designed to assess their ability to deal with a sophisticated smallpox attack in March 1998. The scenario involved an outbreak in California and the Southwest of a genetically-engineered strain of variola similar to one the Soviets had been developing. Officials were unable to contain the smallpox outbreak without large numbers of casualties and could not contain secondary outbreak due to the genetic changes in the virus. Critics of the exercise point out that the virus used in the model was "science fiction," although it pointed to weaknesses in the system. Officials realized "they lacked the knowledge, resources, and stamina to contain or treat a secondary outbreak" of any disease.
A sophisticated smallpox attack might involve the release of genetically-altered variola. A government which has retained smallpox stocks might hire scientists to genetically engineer a more deadly version of variola or a chimera - a genetic hybrid of variola and another virus - neither of which anyone would have immunity to, whether vaccinated or not. Such a virus could cause a secondary outbreak of another disease after a smallpox outbreak.
The government is likely prepared to deal with a small-scale attack perpetrated with variola that has not been genetically altered. Such isolated attacks are more likely than large-scale, sophisticated attacks with genetically engineered viruses: The risks to the public caused by mass-vaccination are far greater than the risk of such a sophisticated attack. While it is unlikely that smallpox will reemerge as a national epidemic in the United States, the acquisition of enough vaccine for all Americans and efforts to change the public health system will help ensure protection in the long run.
References
American Medical Association Working Group for Civilian Biodefense. "Consensus Statement: Smallpox as a Biological Weapon: Medical and Public Health Management." Journal of the American Medical Association 281 (1999): 2127-2137. http://jama.ama-assn.org/issues/v281n22/ffull/jst90000.html [Link current as of August 17, 2002.]
Bradsher, Keith. "Smallpox Vaccine Costlier Than Expected." New York Times 7 November 2001. New York Times On The Web. 29 March 02.
Cohen, Jon. "Smallpox Vaccinations: How Much Protection Remains?" Science 294 (2001): 985.
Donn, Jeff. "Qualms Grow with Bioterror Research." Los Angeles Times Online. 27 January 2002. http://www.latimes.com/news/nationworld/wire/sns-ap-bioterrorism-research0127jan27.story [Link current as of August 17, 2002.]
Fenn, Elizabeth. Pox Americana: The Great Smallpox Epidemic of 1775-82. New York: Hill and Wang, 2001.
Meckler, Laura. "US to Stockpile Smallpox Vaccine." Los Angeles Times Online. 29 November 2001. http://www.latimes.com/news/nationworld/wire/sns-worldtrade-smallpox.story [Link current as of August 17, 2002.]
Miller, Judith, Steve Engelberg, and William Broad. Germs: Biological Weapons and America's Secret War. New York: Simon and Schuster, 2001.
Miller, Judith. "U.S. Set to Retain Smallpox Stocks." New York Times Online. 16 November 2001. http://www.nytimes.com/2001/11/16/international/16GERM.html?searchpv=past7days [Link current as of August 17, 2002.]
Neergaard, Lauren. "Bush Proposes Major Raise for NIH." Los Angeles Times Online. 25 January 2002. http://www.insulinfree.org/society/bush.htm [Link current as of August 17, 2002.]
Nullis, Claire. "Smallpox May Be Kept for Research." Los Angeles Times Online. 17 January 2002. Note: AP archives are available on Lexus/Nexus at your local library.
Ornstein, Charles. "Survivors of the War on Smallpox Fear Their Old Foe." Los Angeles Times online. 6 November 2001. http://www.latimes.com/news/nationworld/wire/sns-worldtrade-smallpox-lat.story [Link current as of August 17, 2002.]
Tucker, Jonathan. Scourge: The Once and Future Threat of Smallpox. New York: Atlantic Monthly Press, 2000.